Effects of Actuated Pelvic Rotation on Sitting Forces and Pressure Distribution.
Jasper Reenalda MSc, Paul van Geffen MSc, Marc Nederhand PhD, MD, Peter Veltink PhD, Bart Koopman PhD, Michiel Jannink PhD, Maarten IJzerman PhD, Hans Rietman PhD, MD.
Abstract
An experimental simulator chair containing a mechanical concept for independent pelvic rotation combined with the possibility to measure sitting load was developed in order to impose dynamic sitting on patients with limited trunk muscle function. Pelvic rotations in the sagittal plane were imposed and the effects on sitting load were investigated. Significant effects of pelvic rotation, with high coefficient of determination were found on sacral load and centre of pressure. It is concluded that the concept for sagittal pelvic actuation is effective to regulate sacral load and centre of pressure, and can be used to control sitting posture. Future experiments, possible with the experimental chair, are discussed.
Keywords
Seating system, pelvic orientation, sitting force, pressure distribution.
BACKGROUND
Patients with limited trunk muscle function, like patients with a spinal cord injury or patients with muscular dystrophy, often adopt a passive and static sitting posture. It is believed that this contributes to many physical problems including the development of pressure ulcers. Sitting acquired pressure ulcers develop mostly on the sacrum and beneath the ischial tuberosities. Prevalence of pressure ulcers, regardless their location is 18.1% in European hospitals (1) and between 12 and 35% in Dutch nursery homes (2). Reported prevalence of pressure ulcers occurring in the ischial, sacral and gluteus region is about 46% (3). In general, healthy people do not suffer physical problems during long term sitting since they regulate body load by continuously changing sitting posture. The inability for patients with limited trunk muscle function to reposition themselves implies that adequate postural change is only possible by the help of others or by automatically adjusting the configuration of the chair (4). However the former usually incorporates a time consuming and physical intensive activity.
We strive to prevent immobility problems by developing a dynamic system, which automatically adjusts sitting posture, similar to healthy sitting behaviour in order to impose dynamic sitting behaviour. Dynamic sitting behaviour is defined as a continuous variation between ‘optimal’ and individualised body postures. Important criteria of dynamic sitting behaviour are postural alignment and proper regulation of the applied forces on the buttocks. A seating device for accurate postural alignment is necessary to meet these criteria.
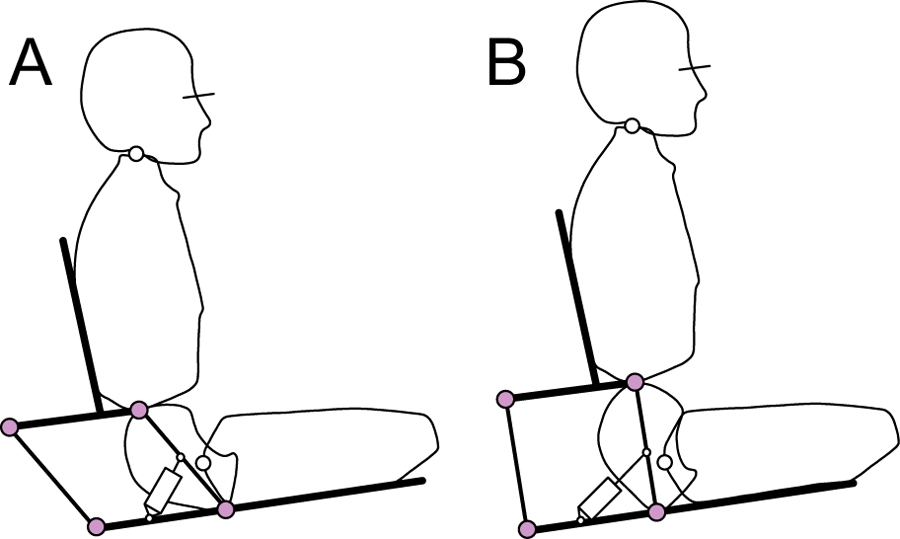 Figure 1: Concept (Click for larger view)
Figure 1: Concept (Click for larger view) Important factors defining sitting posture are the orientation of the trunk, pelvis and thighs. Especially pelvic tilt is crucial for the adopted posture (5). Therefore, chair configurations that regulate proper pelvic alignment, independent from the trunk and the thighs, are important and essential to prevent pressure ulcers and other physical problems such as low back pain and lumbar immobility. We developed an experimental simulator chair, containing a mechanical concept for independent pelvic rotation combined with the possibility to measure sitting load, in order to evaluate the effectiveness of the pelvic control.
Research Question
The objective of this paper is twofold. First a concept for independent pelvic rotation will be described. Second an investigation of the effects of actuated pelvic rotation on pressure distribution and the orientation of sitting forces will be reported. With the concept for independent pelvic rotation we try to answer the research question whether the orientation of sitting forces and pressure distribution can be regulated by imposing actuated pelvic rotation in the sagittal plane.
METHOD
Independent Pelvic Rotation
Figure 1A shows a mechanical concept for independent pelvic rotation. This concept is based on a parallelogram on which the back support is fixed. The configuration of the parallelogram imposes pelvic tilt and is actuated from the seat frame. Configurations enforcing pelvic posterior tilt and pelvic anterior tilt are shown in figures 1A and 1B.
Subjects
Twenty healthy male subjects (age 23 ± 2 years, weight 75 ± 8 kg, Length 1.84 ± 0.05 m) were recruited for this study. Prior to the experiment, all subjects read and signed and ‘informed consent’ in which the objective and experimental protocol was explained. The protocol was approved by the local Medical and Ethical Committee (METC).
Experimental Setup
To investigate the effects of pelvic rotation on the mechanical loading of the buttocks, we developed an experimental simulator chair containing the concept for independent pelvic rotation (figure 2A). For accurate 3D measurements of sitting forces, six uni-axial force sensors (Tension & Compression Load Cell, FUTEK, California, USA) were mounted in the seat frame. The operating system for chair actuation and real-time data processing was based on a Matlab/Simulink environment.
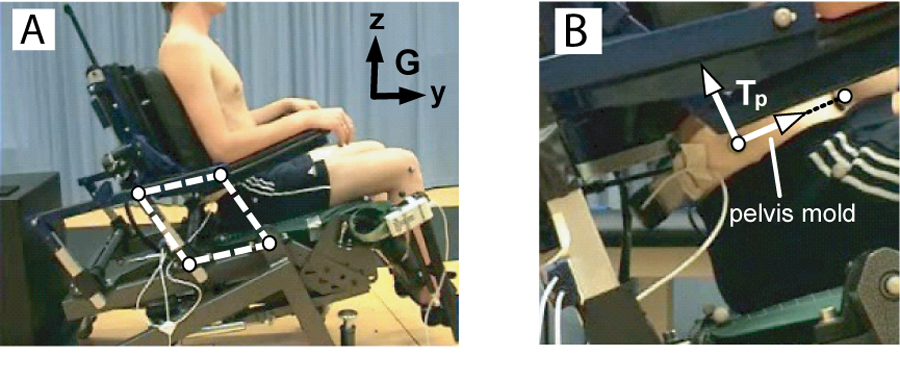 Figure 2: Experimental Setup (Click for larger view)
Figure 2: Experimental Setup (Click for larger view) Pelvic orientation and movement was recorded using an infrared VICON motion capturing system with six cameras. To prevent skin artefacts during pelvic movement a plastic pelvis mold (PM) was shaped around the left and right lateral ischial crest and clamped the Anterior- and Posterior Superior Iliac Spines for optimal fixation. Four reflective markers were placed on the PM to measure pelvic orientation. A Tekscan Comformat pressure mapping device (Teksan Inc, Boston Massachusetts, USA) was placed over the seat and was used to measure pressure distribution.
Protocol
From an initial chair configuration, sagittal pelvic rotation was imposed by actuating the configuration of the parallelogram within a range of 35 degrees relative to the seat. Each measurement involved 2 cycles of actuated pelvic movements with a time period of 30 seconds. Before each trial, two cycles of actuated pelvic rotation were performed to accustom the subject to the pelvic movement and to maintain as passive a possible.
Data analysis
Pelvis marker locations were used to construct a local pelvis coordinate system (Tp) from which we derived pelvic tilt (α) in the sagittal plane. Analogue force data were used to calculate the contact force and point of application (centre of pressure, cp) relative to the seat. Shear- (Fs) and the normal force (Fn) were defined parallel and perpendicular to the seat.
Pressure distribution was derived from the analogue pressure data and was also defined relatively to the seat. To represent tuberal and sacral load, a dispersion index (DI) was calculated. This index relates the interface pressure applied under the sacral area and both tuberosities with the total pressure measured on the seat (Pseat), expressed as a percentage of Pseat. The tuberal and sacral areas were derived within an initial sitting posture and were defined by a 60 mm x 60 mm square surface around its maximal value.
Each trial started with a static reference measurement in which we determined the initial value and ranges for pelvis angle (α) and seat reaction load (cp, Fs, Fn, DItl, DItr and DIs). All quantities were normalized (Δα, Δcp, ΔFs, ΔFn, ΔDItl, ΔDItr and ΔDIs) to percentages of its total range.
RESULTS
Initial values and ranges are presented in table 1. Normalized quantities (dependent variables) were related to Δα (independent variable) and coefficients of determination (r2 ) with accompanying significance were derived.
| Variable | Units | Initial | Range(Δ) |
|---|---|---|---|
α |
[degrees] | 22±5 |
19±2 |
cp |
[mm] | 54±19 |
54±7 |
Fs |
[N/kg] | -0.01±0.36 |
0.70±0.30 |
Fn |
[N/kg] | 7.12±0.53 |
0.65±0.14 |
Ptr |
[Pa/kg] | 184±26 |
34±14 |
Ptl |
[Pa/kg] | 189±23 |
28±12 |
Ps |
[Pa/kg] | 123±24 |
99±29 |
DItr |
[%Pseat] | 8.7±1.2 |
1.7±0.7 |
DItl |
[%Pseat] | 8.9±1.1 |
1.4±0.5 |
DIs |
[%Pseat] | 5.8±1.1 |
4.6±1.4 |
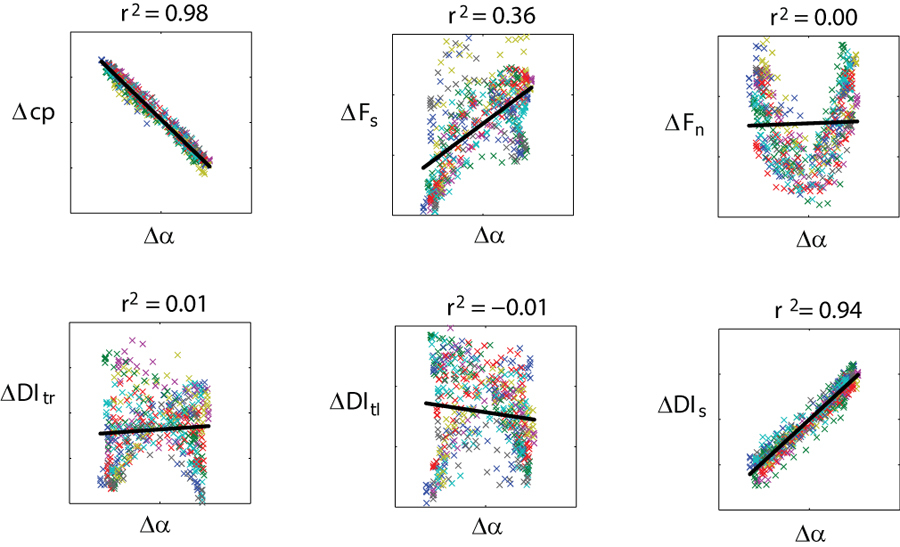 Figure 3: Results (Click for larger view)
Figure 3: Results (Click for larger view) High significant (p < 0.05) coefficients of determination (r2 >0.8) were found for Δcp and ΔDIs (figure 3). No significant correlation was found between ΔFs, ΔFn, ΔDItl, ΔDItr and pelvic orientation.
DISCUSSION AND CONCLUSIONS
Independent control of pelvic orientation is possible with the developed experimental seating system. Actuated pelvic rotation is effective to regulate sacral load and this can be used to control sitting posture. Significant and strongly correlated linear relations were found for pelvic rotation with sacral load and the forces applied within the sacral region. In addition, the displacement of the centre of pressure was significantly correlated to the pelvic orientation. A change in centre of pressure with a range 54 ± 7 mm was observed as a result of pelvic rotation, indicating that the centre of pressure can be controlled by actuating the pelvic orientation. This stresses the importance of the orientation of the pelvis in the determination of the sitting posture.
It is possible to alter sacral pressure distribution with a range of 4.6 ± 1.4% from its initial value of 5.8% indicating an alteration of sacral pressure of up to 79%. However, it is not possible to determine to what extent pressure ulcers can be prevented by this pressure alteration. No clinically usable threshold values are yet determined for the interface pressure or the dispersion index. In addition, as a result of prolonged sitting, pressure ulcers develop subcutaneously (6, 7). Finite element modelling and studies with phantoms have shown that internal stresses in the muscle tissue beneath the bony prominences are higher than the interface pressure between the skin and the sitting surface (8, 9, 10). More research on the internal load as a consequence of the externally applied load is necessary to determine clinically usable thresholds.
No relation was found between pelvic orientation and tuberal load. It is therefore not possible to regulate the tuberal pressure distribution by actuating pelvic orientation in the sagittal plane. In this plane, regulating the tuberal load seems not obtainable because the pelvis is rotated over the ischial tuberosties. As a result there will always be a transfer of load between the seat and the body through the ischial tuberosities. In contrary, the sacrum transfers no load at all when the pelvis is maximally rotated forward. To regulate the sitting load on the ischial tuberosities it is necessary to impose pelvic rotation in the frontal plane. With the seating system it is possible to impose pelvic rotation in the frontal plane in two different ways. First the seat is divided into two parts that can be actuated in height separately. The actuation in height causes a rotation of the pelvis. Second, the seating system is equipped with two actuators in the seat, placed under the ischial tuberosities. The actuators are spaced according to an average inter-tuberal distance (11). In this way, tuberal load can be regulated by actuators in the seat of the experimental chair without changes the posture of the subjects.
It is concluded that the concept for sagittal pelvic actuation is effective to regulate sacral load and centre of pressure, and can be used to control sitting posture. Future experiments should focus on the effects of pelvic rotation in the frontal plane on the sitting load.
References
- Vanderwee, K., Clark, M., Dealey, C., Gunningberg, L., Defloor, T. (2007). Pressure ulcer prevalence in Europe: a pilot study. Journal of Evaluation in Clinical Practice, 13, 227-235.
- Health Council of the Netherlands (1999). Pressure Ulcers. The Hague: Health Council of the Netherlands, publication no. 1999/23.
- Swaine, J., Young, C. (2005). Sitting Acquired Pressure Ulcers: Collecting incidence data in Tasmania. In Proceedings of the 21th International Seating Symposium, Orlando Florida, pp 109-110
- Makhsous, M., et al. (2003). Sitting with adjustable ischial and back supports: biomechanical changes. Spine, 28, 1113-21; discussion 1121-2.
- Hobson, D. A. & Tooms, R. E. (1992). Seated lumbar/pelvic alignment. A comparison between spinal cord-injured and noninjured groups. Spine, 17, 293-8.
- Bouten, C.V.C., Bosboom, E.M.H., Oomens, C.W.J. (1999). The etiology of pressure sores: A tissue and cell mechanics approach. In: Biomedical aspects of manual wheelchair propulsion. L.H.V. Van der Woude et al. (Eds.) IOS Press, (pp. 52-62).
- Bouten, C.V.C., Oomens, C.W.J., Baaijens, F.P.T., Bader, D.L. (2003). The etiology of pressure ulcers: Skin deep or muscle bound. Archives of Physical and Medical Rehabilitation, 84, 616-619.
- Staarink, H.A.M. (1995). Sitting posture, comfort and pressure. Delft University Press, Delft, The Netherlands.
- Oomens, C.W.J., Bressers, O.F.J.T., Bosboom, E.M.H., Bouten, C.V.C., Bader, D.L. (2003). Can loaded interface characteristics influence strain distributions in muscle adjacent to bony prominences? Computer Methods in Biomechanics and Biomedical Engineering, 6(3), 177-180.
- Gefen, A., Levine, J. (2007). The false premise in measuring body-support interface pressures for preventing serious pressure ulcers. Journal of Medical Engineering & Technology, 31(5), 375-380.
- Linder-Ganz, E., Shabshin, N., Itzchak, Y., Gefen, A. (2006). Assessment of mechanical conditions in sub-dermal tissues during sitting: A combined experimental-MRI and finite element approach. Journal of Biomechanics, 40(7):1443-1154.
Acknowledements
This study was partly funded by the Dutch Ministry of Economic Affairs, SenterNovem. The authors would like to thank the engineering company Demcon (Oldenzaal, the Netherlands) for their contribution in the design and development of the experimental simulator chair.
Author Contact Information
Jasper Reenalda MSc, Roessingh Research and Development, ‘t Roessingh Centre for Rehabilitation. Roessinghsbleekweg 33B, 7522 AH Enschede, the Netherlands. Telephone: +31 53 48755726, Email: j.reenalda@rrd.nl